Case Report: Glioblastoma Multiforme, Male, age 61 and a 34-Day Miracle
61 year-old man, told he would be dead within a month after catastrophic recurrence, initiated fenbendazole and watched his tumors disappear in thirty-four days.

Reprinted from Fenbendazole Can Cure Cancer

April 27, 2026
Fenbendazole Can Cure Cancer presents Case Reports of people who have treated their own cancers, along with other articles to help understand how fenbendazole works to treat cancer. Previous articles covering other cancers are in the Archives link.
Glioblastoma multiforme (GBM) is the most common and most aggressive primary malignant brain tumor in adults, accounting for roughly half of all primary malignant brain tumors diagnosed each year (Nahm et al., 2023; StatPearls, 2024). Its infiltrative architecture makes complete surgical removal biologically impossible, and its heterogeneous tumor microenvironment — marked by high mutational burden, immune privilege, and abundant vascular endothelial growth factor expression — has defeated virtually every novel therapeutic strategy attempted over the past half-century (StatPearls, 2024; Supple, 2026).
The gold-standard treatment regimen — maximal safe surgical resection followed by concurrent temozolomide chemotherapy and fractionated radiotherapy (the Stupp protocol), with bevacizumab reserved for recurrent disease — has yielded a median overall survival of approximately 15 months in clinical trial populations and roughly 11 months in real-world practice (Fekete et al., 2023; Nahm et al., 2023). Recurrence is not a risk — it is a near-certainty, typically occurring within six to nine months of initial treatment. Once disease recurs, the median survival from progression is just three to nine months, and subsequent treatment options yield rapidly diminishing returns (Nahm et al., 2023).
For these reasons, GBM has been called the “emperor of all cancers” — a term earned not by its frequency but by its near-total defiance of medical intervention. It is against this backdrop that the case of SM must be understood. What follows is not a statistical outlier in a spreadsheet; it is a man who rebuilt his garden, attended his son’s wedding, and is still casting a fishing line — two years after his oncologist had no more treatments to offer.
Case Report
PERSONAL PROFILE
SM is a sixty-one-year-old male at the time of initial diagnosis, a self-described “country boy” whose avocations — hunting, fishing, and gardening — required the physical and cognitive capacity that GBM would systematically strip from him before fenbendazole intervened. His case was reported to this publication by his sister, MM, who served as the architect of his adjunctive treatment strategy.
INITIAL PRESENTATION AND DIAGNOSIS
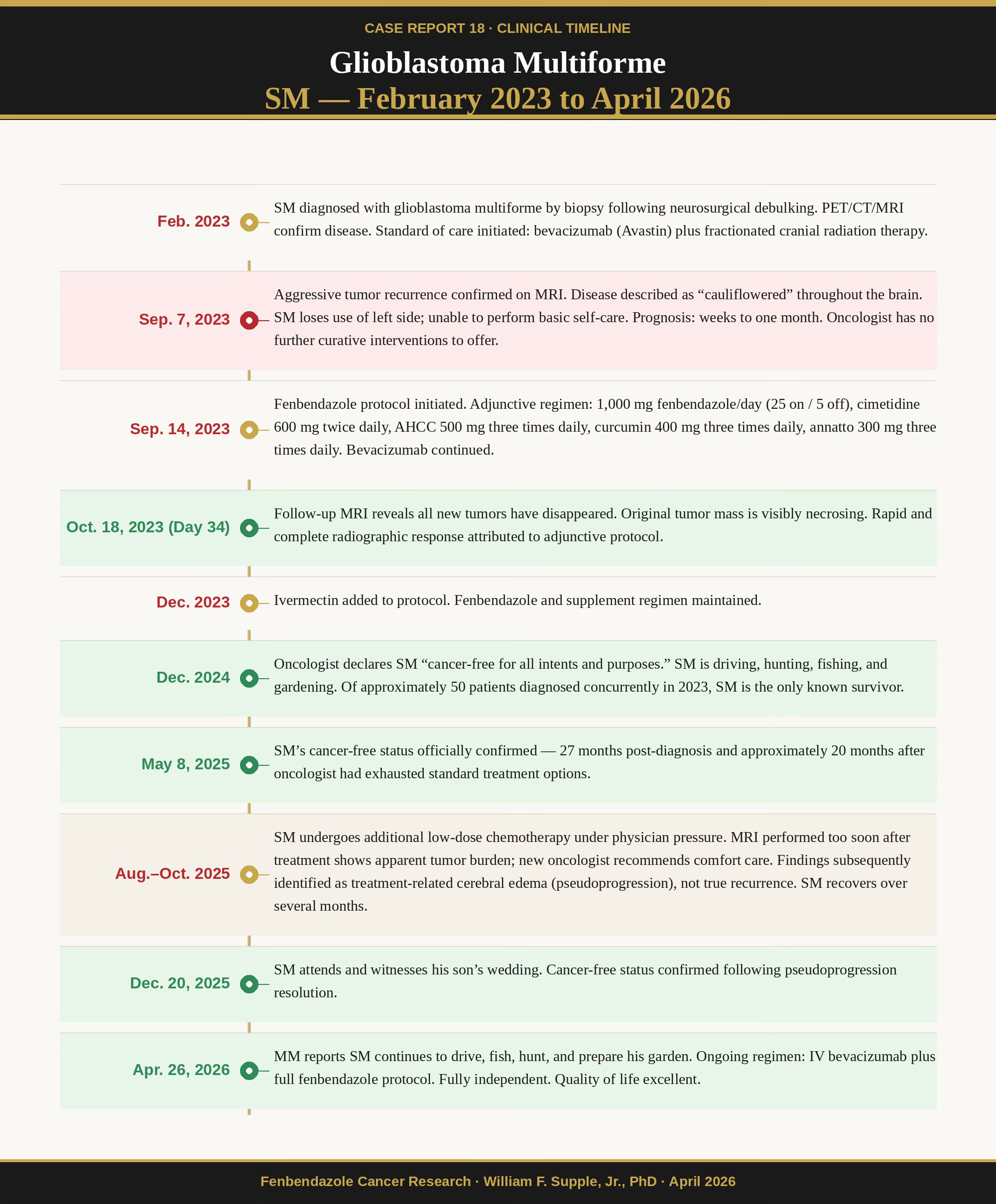
In February 2023, SM received a confirmed diagnosis of glioblastoma multiforme. Comprehensive multimodal imaging — including PET, CT, and MRI — delineated the tumor burden, and the diagnosis was confirmed histopathologically by biopsy of tissue resected during urgent neurosurgical debulking. Following recovery, SM entered the standard-of-care pathway, receiving bevacizumab (Avastin) and a full course of fractionated cranial radiation therapy.
RECURRENCE: SEPTEMBER 7, 2023
Seven months after diagnosis — precisely within the expected window of recurrence — SM’s GBM returned with what his sister described as cauliflower-like proliferation throughout the brain. The clinical consequences were severe: SM lost motor function on his left side, rendering him unable to perform basic activities of daily living, including dressing himself. His oncologist, faced with a rapidly progressing recurrent GBM in a patient already on bevacizumab, had no curative options to offer. The prognosis at this juncture was weeks to months. SM’s own assessment was stark: “I have nothing to lose — I’ll be dead in a month.”
INITIATION OF FENBENDAZOLE PROTOCOL:
SEPTEMBER 14, 2023
One week after his devastating recurrence was confirmed, MM persuaded SM to begin an adjunctive fenbendazole-based regimen. The complete protocol is detailed below:

RESPONSE: OCTOBER 18, 2023 — THIRTY-FOUR DAYS LATER
The MRI obtained thirty-four days after fenbendazole initiation delivered results that stunned the treating team. All newly formed tumor manifestations had disappeared. The original, established tumor mass was visibly necrosing — dying from within. The rapidity and completeness of this response, occurring within a single month in a patient whose cancer had been progressing aggressively on bevacizumab, points unambiguously to the adjunctive protocol — and most specifically to fenbendazole — as the decisive intervention.
“He’s a country boy that thought I was an idiot for asking him to take dog dewormer for brain cancer, until he was like ‘I have nothing to lose — I’ll be dead in a month.’ It does sound insane unless you’ve read documentation and read the testimonies, but here we are, one of those success stories!”
— MM, SM’s sister and protocol architect
SUSTAINED REMISSION AND QUALITY OF LIFE:
DECEMBER 2024
One year after initiating fenbendazole, SM’s oncologist — a physician who candidly acknowledged he had never before produced a comparable outcome in a GBM patient — declared SM “cancer-free for all intents and purposes.” This assessment was rendered more striking by the oncologist’s acknowledgment that conventional chemotherapy would typically have left a patient in SM’s situation severely debilitated and unable to live independently. Instead, SM was driving, hunting, fishing, and gardening. Of the approximately fifty GBM patients who had been diagnosed alongside SM in 2023, he was, by this point, the sole survivor.
OFFICIAL CONFIRMATION: MAY 8, 2025
SM’s status as essentially cancer-free was formally confirmed on May 8, 2025 — approximately twenty-seven months after initial diagnosis, and nearly twenty months after a recurrence his oncologist could offer nothing further to treat.
UPDATE: APRIL 26, 2026
In a communication received yesterday, MM provided the following update. Following sustained improvement, SM faced pressure from his medical team to undergo another round of low-dose chemotherapy. An MRI performed shortly thereafter showed apparent tumor burden, and a new oncologist delivered the grim assessment that the brain was full of tumors and recommended comfort care only. This proved to be a misdiagnosis: the imaging findings were subsequently attributed to treatment-related cerebral swelling (pseudoprogression), not true recurrence. After several months of recovery from this episode, SM was again confirmed as cancer-free. He attended his son’s wedding on December 20, 2025. He continues to drive, fish, and hunt, and is preparing to start his garden. He remains on continuous IV bevacizumab and the fenbendazole protocol; he experiences fatigue following bevacizumab infusions but maintains independent function and an excellent quality of life.
“He’s driving, fishing, hunting and getting ready to start his garden. He was able to see his son get married December 20, 2025. All good things! He is still doing the IV Avastin along with the fenbendazole protocol we came up with. I am thankful for you and your community. I pray you continue to touch many lives!”
— MM, communication received April 26, 2026
Discussion
The case of SM presents a constellation of features that, individually, are each extraordinarily uncommon in GBM — and their simultaneous occurrence in a single patient strains any explanation that does not include the fenbendazole protocol.
First, consider the baseline trajectory. Recurrent GBM following bevacizumab — which SM had already been receiving — carries a median post-progression overall survival of approximately 3.4 to 3.8 months (Ellingson et al., 2017). SM’s oncologist’s candid admission that he had never generated a comparable success story in this disease, and that his GBM patients routinely succumbed before further treatment was possible, corroborates this statistical reality at the individual clinical level.
Second, consider the temporal relationship. SM’s cancer was progressing on bevacizumab and radiation. Fenbendazole was introduced on September 14, 2023. Thirty-four days later, all new tumors had vanished and the original mass was necrosing. Bevacizumab was the only constant between the two imaging studies; it was already failing. The introduction of fenbendazole — and the accompanying cimetidine, AHCC, and curcumin — is the only variable that changed in the interval between radiographic catastrophe and radiographic remission.
Third, consider the mechanism-outcome alignment. GBM is defined by rapid cell division, aggressive glucose metabolism (Warburg effect), and evasion of immune surveillance. Fenbendazole directly attacks all three: it arrests mitosis via tubulin disruption, starves tumors by suppressing GLUT transporters and HKII, and its companion cimetidine actively restores suppressed immune function and blocks VEGF-mediated angiogenesis. The observed necrosing pattern — tumors dying from within — is precisely consistent with the metabolic starvation and apoptotic cascade that the biochemical literature predicts.
The April 2026 pseudoprogression episode deserves specific comment because it illustrates a critical danger that families and patients must understand. Treatment-related imaging changes — swelling and inflammation that mimic tumor on MRI — are well-documented in GBM following chemotherapy and radiation. A new oncologist unfamiliar with SM’s full history interpreted these changes as frank recurrence and recommended hospice. Had MM and SM not maintained their resolve and sought clarification, a SM might have abandoned his highly effective protocol based on a misread scan. This episode reinforces that imaging findings in GBM patients on aggressive multimodal therapy must always be interpreted in full clinical context, with pseudoprogression as a leading differential, before any therapeutic surrender is contemplated.
Finally, MM’s report that SM’s experience has contributed to six additional individuals achieving cancer-free status underscores the network effect of these case reports. Knowledge shared freely — without institutional gatekeeping, without the requirement for a pharmaceutical sponsor’s approval — saves lives. That is why this publication exists.
Conclusion
GBM kills virtually everyone it touches, and it kills them quickly. SM had every actuarial reason to be dead within a month of his September 2023 recurrence (today is April 27, 2026). The science of benzimidazoles in brain tumors predicted that fenbendazole could work; the clinical record of SM confirms that it did. His oncologist had never seen anything like it. His original patient cohort of approximately fifty people is gone. He is tending his garden in the spring of 2026.
Of course fenbendazole isn’t a guaranteed cure for every instance of GBM or any other cancer in all situations but there is no reason to not include it in any treatment regimen; standard of care or alternative. What the data in SMs case plainly show: that a 34-day interval separated progressive, treatment-refractory GBM from complete tumor necrosis, and that the only substantive change in that interval was the initiation of fenbendazole and its companion agents. The scientific literature tells us exactly how and why that could happen. This case tells us that it did.
We extend our deepest gratitude to MM for her courage, her diligence, and her generosity in sharing this story. And to SM — a country boy who was willing to take a chance on dog dewormer when every other door had closed — we say: keep fishing.
The following is a deeper dive exploration of the potential explanation of the synergistic effect of fenbendazole on the Avastin glioblastoma treatments that SM received.
Bevacizumab (Avastin) – Fenbendazole Synergy
A compelling and mechanistically coherent explanation for SM’s extraordinary response is a synergistic interaction between bevacizumab and fenbendazole operating along complementary and mutually reinforcing anti-angiogenic axes (as detailed in Supple, 2026).
Bevacizumab is a humanized monoclonal antibody that neutralizes circulating VEGF-A, preventing its binding to VEGFR1 and VEGFR2 on tumor endothelial cells and thereby suppressing the dominant pro-angiogenic pathway in GBM (Morin, 2016). Bevacizumab clears circulating VEGF and prevents it from binding to receptors on the surface of endothelial cells, thereby inhibiting angiogenesis  — a mechanism that has produced radiographic response rates of 30–50% in recurrent GBM, though without consistent improvement in overall survival (Morin, 2016).
The critical limitation of bevacizumab monotherapy is well characterized: the ability of glioblastoma to progress during bevacizumab treatment suggests that the tumor may have the ability to adapt and fuel its blood supply without using VEGF-A , with resistance driven by upregulation of alternative angiogenic pathways including fibroblast growth factor 2 (FGF-2) and placental growth factor (PlGF) (Takahashi et al., 2024). Compounding this escape mechanism, preclinical data demonstrate that bevacizumab increases the expression of hypoxic markers and glycolytic proteins including GLUT1, effectively driving tumor cells toward enhanced glucose metabolism as a compensatory survival strategy — precisely the metabolic state that fenbendazole is uniquely positioned to counter. Fenbendazole and its benzimidazole analogues address this liability directly: fenbendazole reduces angiogenesis-related proteins such as HIF-1α, VEGF, and VEGFR2 kinase activity , targeting the same angiogenic apparatus through an independent molecular mechanism (Diao et al., 2021). Computational screening identified mebendazole — the nearest human analogue of fenbendazole — as a direct inhibitor of VEGFR2 kinase, and this finding was confirmed in vitro: mebendazole inhibited VEGFR2 autophosphorylation at 1–10 µM in cultured endothelial cell types that line tumor vasculature (Marzagalli et al., 2023). When bevacizumab neutralizes extracellular VEGF agents while fenbendazole simultaneously suppresses VEGFR2 kinase activity and downstream HIF-1α signaling, the result is a dual blockade of the angiogenic axis — upstream and downstream simultaneously — that neither agent can achieve alone.
Beyond this dual anti-angiogenic action, fenbendazole directly addresses the glycolytic escape response that bevacizumab induces. When bevacizumab-mediated vascular normalization creates intratumoral hypoxia, surviving GBM cells upregulate GLUT1 transporter expression and accelerate aerobic glycolysis through the Warburg pathway to maintain ATP production (Pinheiro et al., 2017). Fenbendazole down-regulates glucose uptake by increasing p53 expression and impacting multiple cellular pathways that act on GLUT and hexokinase II, causing cancer cell starvation and enhancing apoptosis  (Nguyen et al., 2024). This anti-Warburg activity constitutes a precise pharmacological counterpunch to bevacizumab’s known liability: the anti-angiogenic drug starves the tumor of blood supply and inadvertently drives glycolytic reprogramming; fenbendazole then disrupts that reprogramming at the enzymatic level, closing the metabolic escape route.
The clinical plausibility of this combination is further substantiated by the fact that academic oncology has already arrived at the same conceptual pairing using mebendazole as the benzimidazole agent. A Phase I trial (NCT01837862) evaluated the safety of mebendazole in combination with bevacizumab and irinotecan in children and young adults with high-grade glioma, finding no dose-limiting toxicities and an overall response rate of 33%, including two partial responses and one complete response sustained for 10 months  (Krystal et al., 2024). The fact that a formal clinical trial independently arrived at the same mechanistic rationale — benzimidazole plus bevacizumab in high-grade glioma — and demonstrated its safety and preliminary efficacy is not coincidental. It is convergent evidence. SM’s protocol combined these two agents in an adult with recurrent GBM rather than pediatric high-grade glioma, and the result was complete tumor necrosis within thirty-four days. The mechanistic basis for that outcome is no longer speculative — it is grounded in preclinical biochemistry, clinical pharmacology, and now a published Phase I trial.
SMs experience is a compelling argument for the addition of fenbendazole to any standard of care protocol for GBM.
References for Avastin-Fenbendazole Synergy Section
Diao, Q., Yu, L., & Yang, J. (2021). The antitumor potentials of benzimidazole anthelmintics as repurposing drugs. Immune Network, 20(4), e29. https://doi.org/10.4110/in.2020.20.e29
Krystal, J., Hanson, D., Donnelly, D., & Atlas, M. (2024). A phase 1 study of mebendazole with bevacizumab and irinotecan in high-grade gliomas. Pediatric Blood & Cancer, 71(4), e30874. https://doi.org/10.1002/pbc.30874
Marzagalli, M., Fontana, F., Raimondi, M., & Limonta, P. (2023). Emerging perspectives on the antiparasitic mebendazole as a repurposed drug for the treatment of brain cancers. International Journal of Molecular Sciences, 24(2), 1334. https://doi.org/10.3390/ijms24021334
Morin, O. M. (2016). Bevacizumab for glioblastoma: Current indications, surgical implications, and future directions. Neurosurgical Focus, 37(6), E9. https://doi.org/10.3171/2014.9.FOCUS14433
Nguyen, J., et al. (2024). Oral fenbendazole for cancer therapy in humans and animals. Anticancer Research, 44(9), 3725–3735. https://doi.org/10.21873/anticanres.17178
Pinheiro, C., Longatto-Filho, A., Azevedo-Silva, J., Casal, M., Schmitt, F. C., & Baltazar, F. (2017). Metabolic alterations underlying bevacizumab therapy in glioblastoma cells. Oncotarget, 8(24), 38538–38551. https://doi.org/10.18632/oncotarget.21761
Supple, W. F., Jr. (2026). Cancer is a Parasite: Kill it with the Safe, Over-the-Counter Antiparasitic Fenbendazole. Skyhorse.
Takahashi, M., Motegi, H., Shirato, K., Watanabe, S., Takemoto, M., & Aoki, T. (2024). Status of alternative angiogenic pathways in glioblastoma resected under and after bevacizumab treatment. Brain Tumor Pathology, 41(2), 47–56. https://doi.org/10.1007/s10014-024-00481-0